Search API
The Ministry of Health, Wellness, and Nutrition in Saint Lucia recently confirmed a laboratory-positive case of the Chikungunya, marking the first such case on the island since 2021. The patient ully recovered and been discharged.
As of March 6, 2026, local health authorities report no additional cases.
However, enhanced surveillance, contact tracing, and intensified mosquito control efforts are underway to prevent any potential spread. Aedes mosquitoes primarily spread Chikungunya, the same vectors that carry dengue and Zika.
Despite this single case, tourism in Saint Lucia remains robust. the Saint Lucia Tourism Authority reported a record-breaking January 2026, which welcomed 37,691 stay-over arrivals. Saint Lucia continues to attract vacationers seeking its beaches, Pitons, luxury resorts, and eco-adventures.
This growth was primarily driven by an 11% increase in visitors from the United States.
This isolated case comes amid broader regional increases in chikungunya virus activity across parts of the Caribbean and Americas, as noted in alerts from the Pan American Health Organization (PAHO).
The isolated chikungunya case has not triggered widespread PAHO advisories or reduced traveler activity in the Americas in 2026.
Vaccine and prevention recommendations remain important for both travelers and residents.
The chikungunya vaccine (VIMKUNYA) is approved in the United States for individuals aged 12 and older and is recommended for travelers to areas with ongoing chikungunya outbreaks or transmission.
Health authorities in Mayotte, a French overseas department in the Indian Ocean, reported 219 confirmed cases of chikungunya since the beginning of 2026. This increase signifies a notable resurgence of the mosquito-borne viral disease on the island, raising ongoing health concerns, especially following larger outbreaks in nearby territories in 2025.
According to updates from TravelHealthPro surveillance bulletins published by Santé Publique France, most of these chikungunya cases are believed to be locally acquired, due to favorable conditions for the Aedes mosquito vectors.
The current 2026 resurgence appears more concentrated in the southern communes of the main island of Grande-Terre.
After several years of relative calm, Mayotte experienced imported cases linked to significant epidemics in neighboring La Réunion, which reported over 54,000 confirmed local cases in 2025 before declaring the outbreak over in June of that year. Other Indian Ocean islands, such as Mauritius and Madagascar, also contributed to these imported cases.
Locally transmitted cases in Mayotte re-emerged in early 2025, prompting the activation of a travel alert in March 2025.
This ongoing situation highlights the persistent threat posed by climate-sensitive arboviruses in tropical and subtropical regions, where environmental factors and travel can quickly reignite transmission. French authorities are urging both residents and visitors to remain proactive in prevention efforts to curb further spread of the disease.
In a broader context for 2026, the Pan American Health Organization (PAHO) has reported over 23,000 chikungunya cases in the Americas, primarily in Brazil and Cuba.
In the United States, Florida recently confirmed both travel-related and one local case.
As of March 4, 2026, chikungunya vaccines are commercially available at travel clinics in the Americas and Europe.
Spanish health authorities have informed the European Centre for Disease Prevention and Control (ECDC) of a confirmed case of human infection with the swine influenza A(H1N1)v virus.
This case was identified in February 2026 in the autonomous region of Catalonia. The patient remained completely asymptomatic, showing no flu-like symptoms such as fever, cough, or malaise, and has since made a full recovery.
Notably, the individual had no known history of exposure to pigs, pig farms, or contaminated environments, which distinguishes this case from most previous zoonotic infections. As of March 3, 2026, all identified close contacts tested negative, and there was no evidence of secondary transmission.
This marks the fourth human case of swine influenza A(H1N1)v reported in Spain over the past 17 years. Fortunately, there has never been documented human-to-human transmission of the A(H1N1) virus in Spain.
Catalonia, located in the northeast, is one of Spain's most intensive pig-rearing regions and has recently faced separate challenges due to detections of African swine fever in wild boars in the Barcelona area.
The ECDC's Communicable Disease Threats Report (Week 9, 2026) states, "Based on the information currently available, the likelihood of further transmission of variant A(H1N1) linked to this event is assessed to be very low."
According to the latest available data from the U.S. CDC, there have been no confirmed cases of variant swine-origin influenza (A(H1N1)v, A(H1N2)v, or A(H3N2)v) reported for the ongoing 2025–26 flu season.
However, during the 2024–2025 flu season, one confirmed human case of swine-origin variant A(H1N2)v infection was reported in Iowa. The adult patient was hospitalized but made a full recovery.
According to the U.S. CDC, seasonal influenza vaccines for 2026 provide no direct protection against swine-origin variant virus strains seen in recent European cases, as those belong to different genetic lineages.
Italy's 2026 Winter Olympic and Paralympic Games recently concluded successfully with no major public health incidents related to communicable diseases.
According to the latest report from the European Centre for Disease Prevention and Control (ECDC), the Winter Olympic Games, held from February 6 to 22, 2026, across venues in Milan, Cortina d'Ampezzo, and other northern Italian sites. The Paralympic Winter Games took place from March 6 to 15, 2026.
In its Communicable Disease Threats Report, the ECDC confirmed that no major public health events tied to communicable diseases occurred in the context of the Games.
This marks a clean slate for the large-scale mass gathering, which drew athletes, officials, and more than 1 million cumulative attendees from around the world.
The ECDC emphasized that staying up to date with routine vaccinations is essential.

A major study recently published in The Journal of Infectious Diseases details a significant measles transmission event linked to an unvaccinated adult who traveled from Europe to Colorado while infectious with the virus.
This article emphasizes the risks associated with air travel in spreading this highly contagious disease and underscores the essential role of vaccination.
The incident is described as one of the most extensive air travel-related measles transmission chains documented in the United States in recent years, with the virus spreading across flights, airport areas, and beyond.
However, as of March 3, 2026, there is no mandatory measles vaccination policy in the U.S. for domestic or international air travel when a person is departing from a measles outbreak area.
Investigators identified 135 travelers who were exposed through aircraft contact tracing. Ultimately, 15 secondary cases arose among those exposed: 5 during the international flight, 3 on the domestic flight, and 7 at the airport transit area. Additionally, 2 tertiary cases were linked to further community spread.
Notably, 5 of the secondary cases had documentation of at least one prior measles vaccination, indicating that breakthrough infections can occur.
The study's authors conclude that measles transmission can easily occur during travel in enclosed environments such as aircraft cabins, where the virus can remain airborne for up to two hours.
Most health agencies strongly recommend that all travelers aged 6 months and older receive measles vaccinations before international travel.
This outbreak highlights broader concerns about rising measles cases in the U.S. and globally, largely driven by gaps in vaccination coverage.
Public health experts worldwide continue to advocate for routine measles immunization as the most effective prevention strategy against such outbreaks.
On March 2, 2026, the U.S. Centers for Disease Control and Prevention acting director and head of the NIH, Jay Bhattacharya, MD, PhD, posted a video on X promoting the measles vaccine.
"Measles is preventable, and vaccination remains the most effective way to protect yourself and those around you," Dr. Bhattacharya stated.

With Spring Break 2026, travelers seeking safe, healthy alternatives to The Bahamas and Mexico will find Florida's pristine beaches and warm waters highly appealing.
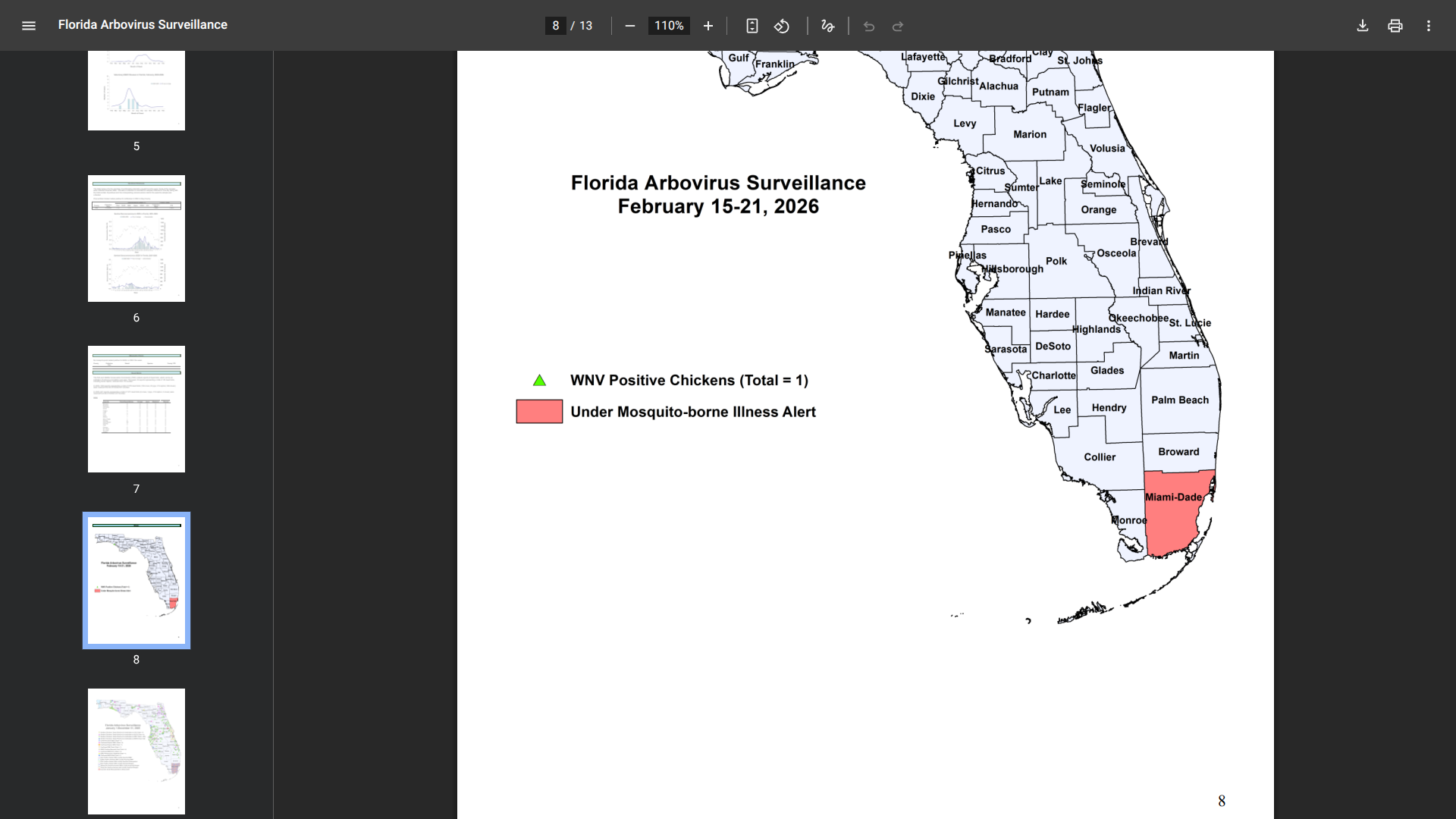
However, Miami-Dade County on Florida's southeast coast is currently under a mosquito-borne illness alert issued by the Florida Department of Health (DOH) due to ongoing travel-associated cases of chikungunya, dengue, and malaria.
As of March 2, 2026, this alert was first expanded in July 2025, after local dengue cases were detected, and was reinforced by a locally acquired chikungunya case reported late last year.
According to the Florida DOH's most recent Arbovirus Surveillance Report (Week 7, covering February 15–21, 2026), there have been 21 travel-associated chikungunya cases statewide, with 13 in Miami-Dade County, all linked to Cuba. In 2025, there was one locally acquired dengue case in Miami-Dade County, which began in December.
So far this year, there have been 14 dengue cases statewide, with 4 occurring in Miami-Dade County, primarily sourced from Cuba.
Additionally, there have been 6 malaria cases statewide, including 3 in Miami-Dade County.
These provisional figures align with earlier reports for 2026 (Weeks 1–5), which also indicated a steady accumulation of imported cases, particularly among residents returning from Cuba and other endemic areas.
The U.S. Centers for Disease Control and Prevention (CDC) notes that Miami-Dade's high volume of international travel continues to serve as a gateway for these pathogens. There is no specific CDC travel alert for Miami-Dade County, but the agency refers travelers to state and local health departments for domestic mosquito surveillance.
Florida's DOH-Miami-Dade and Miami-Dade County Mosquito Control are actively coordinating enhanced surveillance, larval source reduction, and public education efforts. Residents and visitors are encouraged to "Fight the Bite.”
Additionally, the CDC recommends that anyone visiting a disease outbreak area speak with a travel vaccine expert weeks before traveling abroad in 2026.
Updated resources from the CDC on these diseases can be found at cdc.gov/dengue, cdc.gov/chikungunya, and cdc.gov/malaria. Please note that case counts in this report are subject to revision.
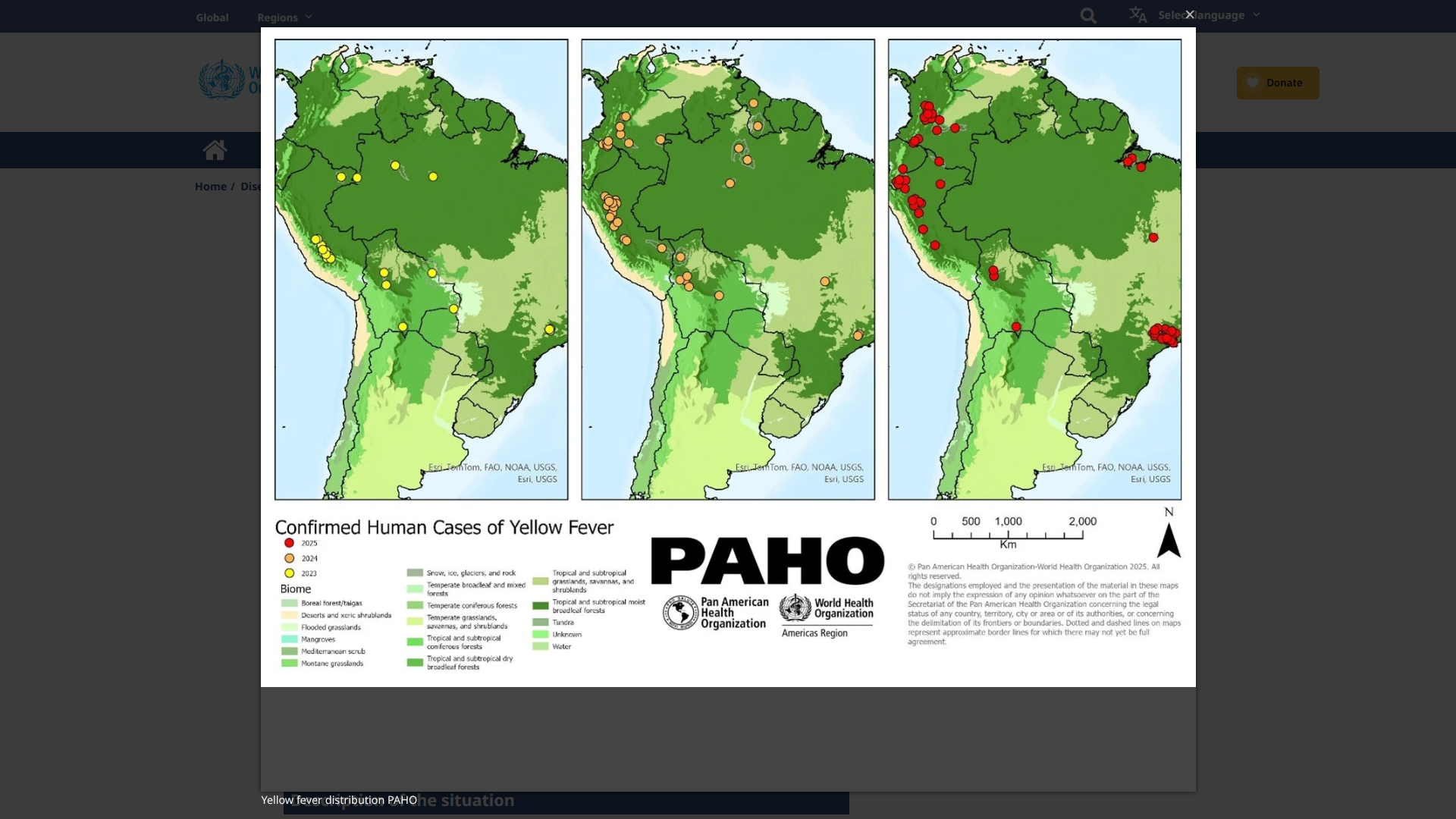
Venezuelan health authorities are addressing a significant resurgence of yellow fever (YF), with 36 laboratory-confirmed human cases since the outbreak began in mid-2025.
As of late February 2026, these mosquito-transmitted cases have been reported across 14 states, indicating a wide geographic spread that surpasses the more localized patterns seen in previous outbreaks.
So far, the disease has remained limited to forest exposures, with no evidence of urban transmission by Aedes aegypti mosquitoes.
Recent public reports have not detailed any related fatalities, though severe YF cases typically have a case-fatality rate of 20–50%.
Venezuela's YF outbreak occurs amid increased activity across the Americas.
In 2024, the region reported 61 confirmed human cases and 30 deaths. By mid-2025, this number surged threefold to over 200 confirmed cases and 85 deaths (with a case-fatality rate of approximately 40%) across several countries, including Brazil, Colombia, Peru, Bolivia, and Ecuador, according to data from the Pan American Health Organization (PAHO).
Subsequent PAHO updates reported even higher totals, with YF outbreaks expanding beyond traditional Amazonian zones into new areas, including Colombia's Tolima department in 2026.
This resurgence serves as a stark reminder of yellow fever's capacity to exploit vaccination gaps in endemic settings.
According to the PAHO, the minimal childhood vaccination coverage—below 80% in Venezuela and several other endemic countries—coupled with climatic factors that favor mosquitoes, has contributed to the intensification of YF outbreaks.
PAHO has repeatedly assessed the risk of yellow fever outbreaks in the Americas as high and has issued multiple epidemiological alerts in 2025, urging mass vaccination in at-risk areas. In response to the current outbreak in Venezuela, emergency vaccination campaigns have been launched, targeting high-priority parishes, particularly in rural and border areas.
The single-dose Stamaril (YF-VAX) vaccine provides lifelong immunity. While proof of yellow fever vaccination is not required for direct arrivals to Venezuela from non-endemic countries like the United States, it is mandatory for travelers aged 1 year and older arriving from or transiting through countries with a risk of transmission, such as Brazil and Colombia.
As of March 2, 2026, the U.S. Centers for Disease Control and Prevention strongly recommends vaccination for most travelers visiting areas below approximately 2,300 meters in elevation, including popular sites like Angel Falls. In the U.S., the YF-VAX vaccine is commercially offered at travel clinics.
However, it is generally not recommended to vaccinate for travel limited to major cities such as Caracas or Valencia.
Separately, the U.S. Department of State maintains a Level 4: Do Not Travel advisory for Venezuela, citing severe risks to visitors in March 2026.

The Dominican Republic has reported a promising decline in certain infectious diseases early in the year, particularly leptospirosis.
This trend suggests improved public health measures and a potentially safer environment for residents and travelers during Spring Break 2026.
According to the Ministry of Public Health's epidemiological surveillance data published on February 19, 2026, confirmed leptospirosis cases showed a clear downward trend during the first five weeks of 2026 compared to the same period in 2025.
There were 17 confirmed cases of leptospirosis in 2026, down from 28 in the equivalent timeframe in 2025.
Leptospirosis remains a concern for the 11 million expected travelers to the Dominican Republic, as it can be contracted through contact with water or soil contaminated by animal urine, especially in rural or flood-prone areas.
This positive trend highlights the effectiveness of intensified efforts by the Ministry of Public Health and Provincial Health Directorates to limit transmission, reduce complications, and prevent fatalities from the disease. Authorities have enhanced active surveillance for febrile illnesses, expanded sample collection, and ensured prompt reporting.
The 2026 data suggest that these proactive measures are helping reduce the number of cases.
Other priority diseases under surveillance also showed favorable trends in 2026.
The number of mosquitoes transmitted Dengue fever cases remained low, with 6 reported, for a cumulative total of 30 cases year-to-date. The provinces with the highest Dengue incidence included Valverde, Elías Piña, La Altagracia, Duarte, San Juan, and Monte Cristi.
Additionally, 17 Malaria cases have been recorded for 2026, primarily concentrated in Guayabal and San Juan.
Furthermore, respiratory virus activity has also trended downward at the start of the year.
However, there is still some circulation of respiratory syncytial virus and influenza, including the A(H3N2) subtype, indicating a prolonged respiratory season with co-circulation of multiple agents and varying peaks.
While the data reflect only the early part of the year, the decline in leptospirosis and the stability of other vector-borne and infectious diseases offer encouraging signs for public health in the Dominican Republic.
According to the U.S. Centers for Disease Control and Prevention (CDC), travelers to the DR are still advised to follow standard precautions, such as avoiding untreated freshwater exposure and using insect repellent.
The CDC also advises staying informed about travel vaccine options.
