Search API

The Florida Department of Health (FDH) published its Arbovirus Surveillance update #23, disclosing that mosquito-borne diseases, such as Dengue, continue to be detected in international travelers and Floridians.
On June 7, 2025, FDH reported 88 cases of Dengue fever among individuals who had traveled internationally, with 40 cases from Cuba.
Last year, Florida reported 1,016 travel-associated dengue cases, primarily among travelers from Brazil, Cuba (567), and Puerto Rico.
So far in 2025, one locally acquired dengue case (DEN-3) has been reported in Miami-Dade County. In 2024, 91 locally acquired dengue cases were reported from ten counties, with Miami-Dade leading the way with 50 cases.
Since the state of Florida has identified 14 mosquito species as vectors of infectious diseases that can transmit to humans, one country has recently taken action to protect its residents by reducing the population of mosquitoes and their habitats.
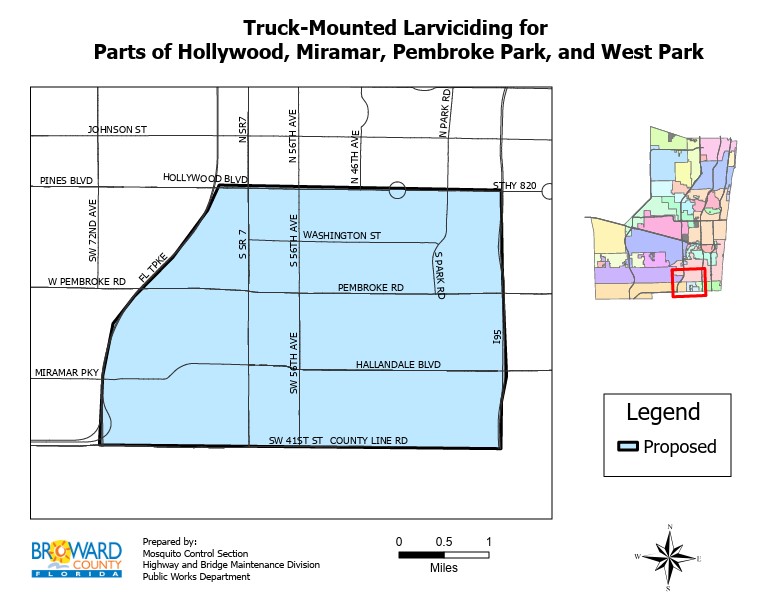
On May 1, 2025, Broward County's Mosquito Control Section announced it began spraying larvicide in areas of Hollywood, Miramar, Pembroke Park, and West Park as a proactive measure to kill the larvae of Aedes aegypti and Aedes albopictus mosquitoes, known to potentially spread diseases such as Dengue, yellow fever, and chikungunya.
According to the County, the larvicide, VectoBac WDG, is not harmful to humans, pets, bees, aquatic habitats, or environmentally sensitive areas. The active ingredient is Bacillus thuringiensis israelensis (Bti, strain AM6552), a naturally occurring, biodegradable bacterial mosquito larvicide.
While this area of Broward County is limited, and local cases of Dengue and malaria have been detected in other Florida counties, this effort is a good step in reducing the number of preventable diseases in 2025.
One of North America's favorite vacation destinations, located just 193 miles east of South Florida, accessible by boat or plane, has been informed by Canada to 'Exercise a high degree of caution.'
On June 3, 2025, Canada affirmed that the Commonwealth of The Bahamas is experiencing a high level of civil unrest, especially in Nassau and Freeport.
The Bahamas is an island country located in the Atlantic Ocean, welcoming approximately 11 million visitors in 2024, many of whom came from Canada and the United States.
Amongst the various warnings, Canada states that the water sports rental industry in the Bahamas is poorly regulated, and reputable operators are limited. Boating accidents occur frequently, particularly on jet skis.
Canada offers the following advice to vacationers: Only rent water sports equipment from reputable, registered operators. Ensure that proper training is provided before using the equipment, and verify that beach and aquatic equipment is safe and in good condition.
The U.S. State Department has also issued a Level 2: Exercise Increased Caution travel advisory for The Bahamas.
Similar to Canada, the U.S. Embassy in Nassau issued a Security Alert on April 9, 2025, advising U.S. citizens of the risks associated with renting jet skis in The Bahamas.
The Embassy wrote, Nassau jet ski operators have raped and sexually assaulted two U.S. citizen women in 2025, and three rapes were reported in 2024.
Women victims reported that male jet ski operators picked them up from downtown Nassau and Paradise Island beaches. This includes the area from Junkanoo Beach to Saunders Beach and Cabbage Beach.
The victims said they were raped and assaulted on isolated islands near New Providence.
Furthermore, due to security risks, U.S. government employees working in The Bahamas are prohibited from renting and using jet skis on New Providence and the Paradise Islands.
From a health perspective, mosquito-transmitted disease reporting from The Bahamas appears lacking.
While the entire Region of the Americas, including the Caribbean countries, set records for Dengue virus infections in 2024, The Bahamas didn't report any cases. Nor has it reported any in 2025.
Which leads to questions about the number of Chikungunya, Malaria, and Zika infections vacationers experience following a Bahamas vacation.
However, the U.S. CDC did include The Bahamas in a recent measles outbreak alert.
Therefore, when scheduling a quick trip to enjoy the warm waters of the Caribbean in June 2025, vacationers should heed the advice from these government agencies and exercise caution.

As thousands of French vacationers plan their summer holiday to visit islands in the Indian Ocean, a mosquito-transmitted disease has become a significant health nuisance in 2025.
To notify international travelers, the U.S. Centers for Disease Control and Prevention (CDC) recently reissued a Level 2 Travel Advisory regarding chikungunya outbreaks in several countries in the region, including Kenya, Madagascar, Mauritius, Mayotte, Réunion, Somalia, and Sri Lanka.
Numerious cases of Chikungunya, both imported and local, have been detected in these vacation destinations.
As of June 10, 2025, the CDC writes, 'Most people infected with the chikungunya virus develop some symptoms. You can protect yourself from disease by preventing mosquito bites, which includes using insect repellent, wearing long-sleeved shirts and pants, and staying in places with air conditioning or that have screens on the windows and doors.
Additionally, vaccination is recommended for travelers who are visiting an area with a chikungunya outbreak. Two chikungunya vaccines are approved for use in the United States, which are commercially available at clinics and pharmacies.

The World Health Organization (WHO) today announced that the Republic of Sudan's Khartoum State is facing an infrastructure breakdown and severe constraints on access to healthcare.
Since May 2025, there has been a rapid increase in cholera cases in Khartoum State, with over 16,000 cumulative cases and 239 deaths reported.
Effective as of June 10, 2025, a 10-day reactive oral cholera vaccination (OCV) campaign was launched in five localities to protect more than 2.6 million people aged 1 year and above from cholera infection, interrupt transmission, and help contain the ongoing cholera outbreak.
WHO Representative in Sudan, Dr Shible Sahbani, commented in a press release, "The vaccines will help stop cholera in its tracks as we strengthen other response interventions."
Khartoum is the capital city of Sudan, with over 7 million residents, located adjacent to the Nile rivers.
The WHO's Global Cholera and Acute Watery Diarrhoea Dashboard was updated in June 2025, indicating that over 224,000 cholera cases and 2,800 related fatalities were reported from 26 countries this year.
Cholera is a vaccine-preventable disease caused by consuming food or water contaminated with the bacterium Vibrio cholerae. It poses a global threat to public health.
As of June 12, 2025, OCV remains in limited supply worldwide, except for the United States.
The Canadian government has issued an updated travel advisory for the Republic of Costa Rica, urging visitors to stay vigilant due to increasing civil unrest and natural hazards.
Published on June 9, 2025, the exercise a high degree of caution travel advisory also notes a rise in localized crime that may come as a surprise to tourists.
This advisory is essential, as Costa Rica attracts thousands of Canadians each year. Approximately 143,000 Canadians visited in the first four months of 2025, with an average stay of 14 nights.
From a health risk perspective, the U.S. Centers for Disease Control and Prevention (CDC) advises that visitors may be exposed to mosquito-transmitted infectious diseases, such as chikungunya, dengue, malaria, and Zika, in June 2025.
Additionally, the Costa Rica Ministry of Health has reported an outbreak of Bordetella pertussis (whooping cough) in the Tibas district of San José.
The CDC recommends checking the travel vaccine list and seeing a healthcare provider at least a month before visiting Costa Rica.
The U.S. Embassy in Costa Rica and the UK NHS have also issued recent health alerts when visiting this Central American travel favorite.



According to an analysis recently published by the U.S. Centers for Disease Control and Prevention (CDC), fewer infants were admitted to hospitals struggling to breathe from Respiratory Syncytial Virus (RSV) last season.
This positive trend was announced in the MMWR (74(16);273–281) on May 8, 2025, following the approval of RSV vaccines and antibody treatments for the 2024-2025 season.
Data from the RSV-Associated Hospitalization Surveillance Network (RSV-NET) and New Vaccine Surveillance Network (NVSN) showed infants aged 0–7 months (eligible for protection with maternal vaccination or nirsevimab), 2024–25 RSV-associated hospitalization rates were lower compared with the 2018–20 pooled rates.
The most significant estimated rate reduction was observed among infants aged 0–2 months (RSV-NET: 52%, 95% CI = 49%–56%; NVSN: 45%, 95% CI = 32%–57%) and during peak hospitalization periods (December–February).
In a sensitivity analysis of the NVSN surveillance site in Houston, Texas, where the RSV season began before vaccine and antibody treatments were available, the effect was even more pronounced, with a 71% drop in infant hospitalizations.
The findings suggest the importance of protecting infants born during the RSV season through either maternal vaccination during pregnancy or nirsevimab (Beyfortus) administration in the first week of life, ideally during the hospitalization for birth.
