Search API
Diakonos Oncology Corporation announced that the U.S. Food and Drug Administration (FDA) has granted Fast Track designation for the company’s unique dendritic cell vaccine (DCV) for pancreatic ductal adenocarcinoma.
On July 15, 2024, the Houston-based company confirmed that DCVs are made with a patient’s dendritic cells and a tumor sample.
These highly differentiated double-loaded dendritic cell vaccines activate robust cytotoxic TH1 cell signaling pathways that initiate a natural immune response to target and eliminate cancer cells. This is achieved without any genetic modification of the patient’s immune cells, which greatly simplifies the manufacturing process and significantly reduces costs compared to leading cell therapy approaches.
“This second FDA Fast Track designation of our autologous dendritic cell vaccines for pancreatic cancer is another acknowledgment of the incredible potential of this innovative immunotherapy for treating the most deadly cancers,” said Mike Wicks, Diakonos CEO, in a press release.
Pancreatic ductal adenocarcinoma is the most common pancreatic cancer. In 2024, an estimated 51,750 people will die, and 66,440 will be newly diagnosed.
FDA Fast Track designation is intended to speed the development and review of drugs that show early clinical promise in treating severe or life-threatening conditions.


During today's U.C. CDC Clinician Outreach and Communication Activity call, the presentation offered insights regarding the multi-year Highly Pathogenic Avian Influenza (HPAI) (H5N1) virus outbreak in the United States.
As of July 16, 2024, the HAPI virus is widespread among wild birds and continues to cause outbreaks in poultry and spillover to mammals, including dairy cattle.
To date, three human cases of HPAI A(H5N1) virus infection have been identified in dairy farm workers in the U.S.
The CDC team wrote, 'The risk to the public from HPAI A(H5N1) viruses is low. However, people with job-related or recreational exposure to infected birds or animals, including dairy cattle, are at greater risk of HPAI A(H5N1) virus infection.
As of July 2024, the U.S. government has invested hundreds of millions of dollars in funding avian influenza vaccines and clinical candidates that could be deployed during a pandemic.

New data published by the World Health Organization (WHO) highlights brighter spots in global immunization coverage. On July 15, 2024, the WHO wrote the steady introduction of new and under-utilized vaccines, including vaccines targeting human papillomavirus (HPV), has produced positive results.
About 85% of people will get an HPV infection in their lifetime.
For example, the share of adolescent girls globally who received at least one dose of the HPV vaccine, which protects against cervical cancer, increased from 20% in 2022 to 27% in 2023.
The use of the single-dose HPV vaccine schedule also helped boost vaccine coverage.
Strong introductions in countries such as Bangladesh, Indonesia, and Nigeria primarily drove this increase.
However, HPV vaccine coverage is well below the 90% target to eliminate cervical cancer as a public health problem, reaching only 56% of adolescent girls in high-income countries and 23% in low- and middle-income countries.
"The HPV vaccine is one of the most impactful vaccines in Gavi’s portfolio, and it is incredibly heartening that it is now reaching more girls than ever before,” said Dr. Sania Nishtar, CEO of Gavi, the Vaccine Alliance, in a WHO press release.
“With vaccines now available to over 50% of eligible girls in African countries, we have much work to be done, but today, we can see we have a clear pathway to eliminating this terrible disease.”
New insights suggest innovative marketing programs are needed to expand HPV vaccine uptake.
A recent poll of over 400,000 users of UNICEF’s digital platform for young people, U-Report, revealed that over 75% are unaware or unsure of what HPV is, underscoring the need for better vaccine accessibility and public awareness.
When informed about the virus, its link to cancers, and the existence of a vaccine, 52% of respondents indicated they want to receive the HPV vaccine but are hindered by financial constraints (41%) and lack of availability (34%).
As of July 2024, various HPV vaccines were available worldwide.
In the United States, the CDC recommends two doses of HPV vaccine for all adolescents at age 11 or 12 years.

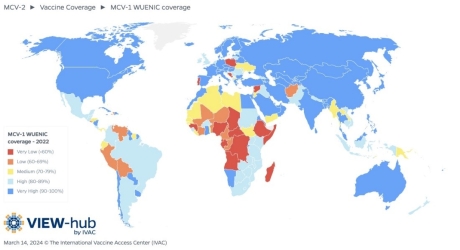
New data published today by the World Health Organization (WHO) revealed that over the last five years, measles outbreaks have hit 103 countries.
In 2023, nearly 35 million children had no or only partial measles protection.
In July 2024, the U.S. CDC listed the top ten international measles outbreaks led by Azerbaijan, Kazakhstan, Iraq, and India. In the United States, the CDC reported 167 measles cases in 24 jurisdictions this year.
On July 15, 2024, the WHO confirmed that only 83% of children worldwide received their first dose of a measles vaccine through routine health services, while the number of children receiving their second dose reached 74%.
These WHO figures fall short of the 95% coverage needed to prevent measles outbreaks.
“Measles outbreaks are the canary in the coal mine, exposing and exploiting gaps in immunization and hitting the most vulnerable first,” said Dr. Tedros Adhanom Ghebreyesus, WHO Director-General, in a press release.
“This is a solvable problem."
"Measles vaccine is cheap and can be delivered even in difficult places. WHO is committed to working with all our partners to support countries in closing these gaps and protecting the most at-risk children as quickly as possible.”
The CDC confirmed in 2024 that if you are unsure if you or your travel companions are fully protected against measles, schedule an appointment to see your clinician at least six weeks before traveling so that you have enough time to get vaccinated with an MMR vaccine.


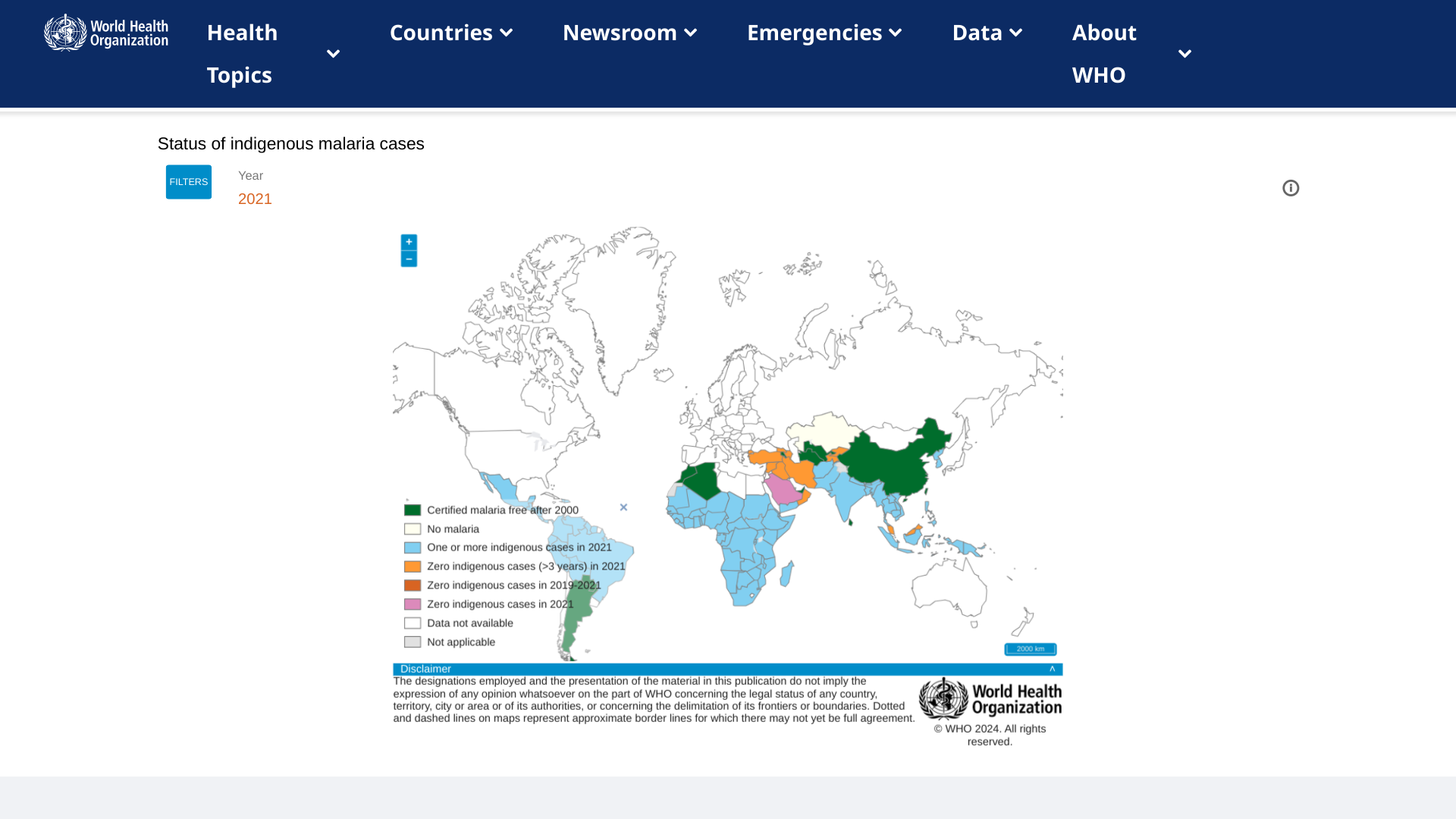
Today marks the official rollout of the newly approved R21/Matrix-M™ malaria vaccine, co-developed by the University of Oxford and Serum Institute of India (SII), which has committed to producing 100 million vaccines.
This malaria vaccine utilizes Novavax’s Matrix-M™ adjuvant technology.
The first official vaccination is scheduled for July 15, 2024, in Abidjan, Côte d’Ivoire, and it will be subsequently introduced in 38 districts across the country.
According to a press release, 15 African countries will introduce malaria vaccines with Gavi support in 2024. These countries plan to reach around 6.6 million children with the malaria vaccine in 2024 and 2025.
John Jacobs, President and Chief Executive Officer of Novavax Inc., commented, "The introduction of the R21/Matrix-M™ malaria vaccine in Côte d'Ivoire marks a breakthrough in the fight to protect vulnerable children against a leading cause of death across the region while reinforcing our mission to create innovative vaccines that improve public health."
"Novavax is proud of the contribution of our Matrix-M™ adjuvant in this vaccine and in making this moment possible, and value our continued collaboration with the University of Oxford and SII, as well as the lifesaving work of WHO, Gavi, and UNICEF.”
R21/Matrix-M is a low-dose, highly effective, and affordable vaccine that can be manufactured quickly and scale. Ghana, Nigeria, Burkina Faso, and the Central African Republic have approved the new vaccine, and many others are preparing to receive shipments.
Malaria vaccines are currently unavailable in the United States.
Novavax, based in Gaithersburg, MD., U.S., promotes improved health by discovering, developing, and commercializing innovative vaccines to help protect against serious infectious diseases.
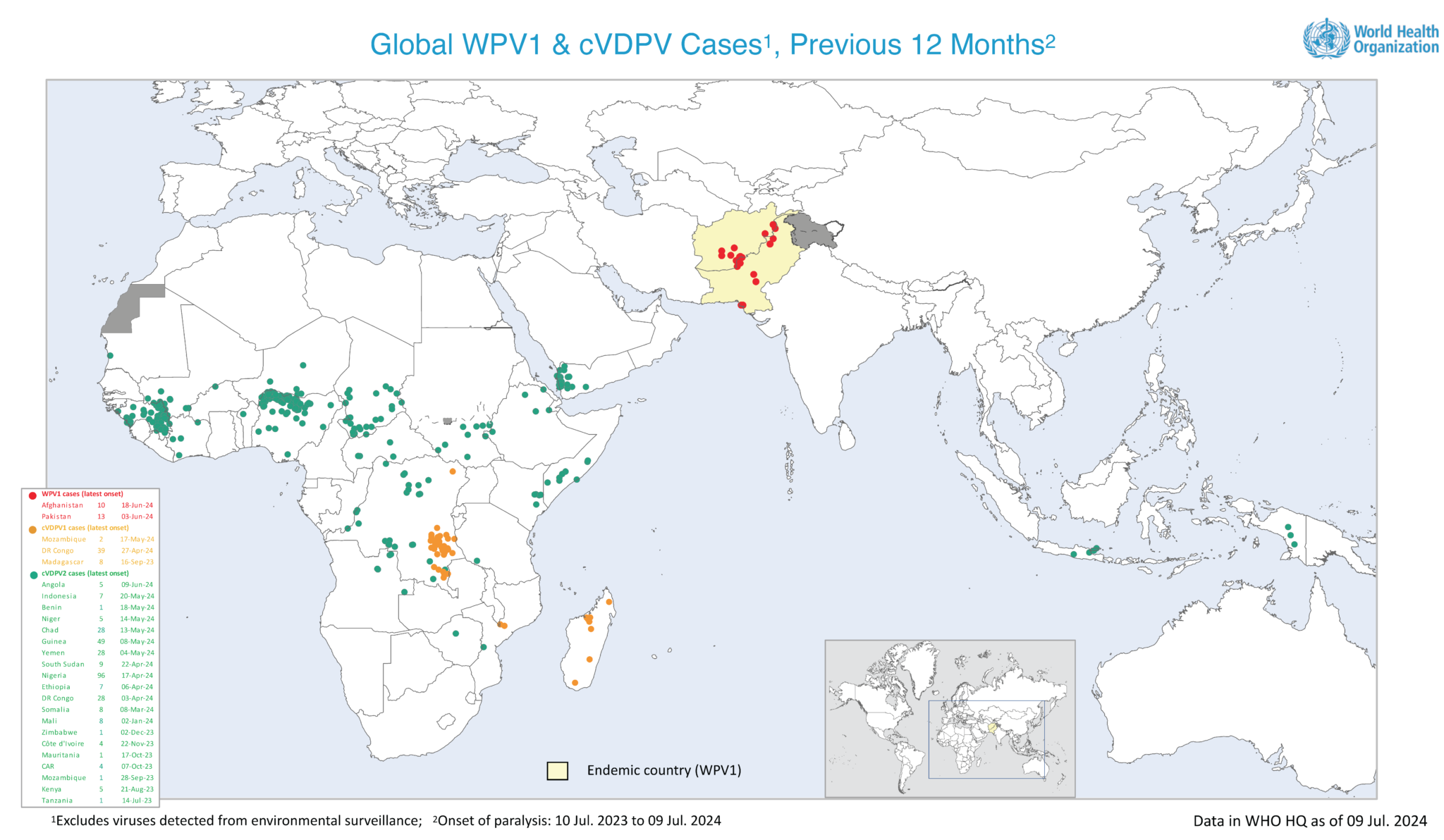
According to the Global Polio Eradication Initiative (GPEI), a joint Polio Independent Monitoring Board and Transition Independent Monitoring Board meeting will be held in Geneva, Switzerland, beginning July 15, 2024.
The goal of the meeting is to assess the challenges of eliminating polio in the endemic and outbreak countries.
Unfortunately, the GPEI reported three additional wild poliovirus type 1 (WPV1) cases in Afghanistan last week, bringing the country's total for 2024 to nine.
In 2023, Afghanistan reported six WPV1 cases.
In this region, Pakistan, which is also fighting the speed of poliovirus, reported eight new WPV1 environmental detections last week.
In addition to these polio disclosures, the U.S. CDC says to interrupt poliovirus transmission, a renewed focus on increasing routine immunization coverage in endemic areas and implementing higher-quality supplementary immunization activities is necessary.
Over the last decade, about 10 billion doses of oral polio vaccine were administered worldwide, reports the GPEI.
The CDC's Global Polio Travel Advisory (May 2024) recommends that before visiting any of the 34 destinations, adults who completed the full, routine polio vaccine series may receive a single, life booster dose of polio vaccine.
In the United States, polio vaccines are generally available at pharmacies and travel clinics.